TBIBANK GRAND ROUNDS
Elise Elbourn
Leanne Togher
Joanne Steel
Emma Power
Davida Fromm
Brian MacWhinney
These materials are provided to students and clinicians who wish to improve their understanding of language-related problems accompanying traumatic brain injury (TBI). None of these materials should be copied or used anywhere outside of these web pages. In particular, none of the videos should be download or copied and placed anywhere else. Users should adhere to the Ground Rules for use of TalkBank data.
INTRODUCTION
Leanne Togher
Joanne Steel
Emma Power
Davida Fromm
Brian MacWhinney
These materials are provided to students and clinicians who wish to improve their understanding of language-related problems accompanying traumatic brain injury (TBI). None of these materials should be copied or used anywhere outside of these web pages. In particular, none of the videos should be download or copied and placed anywhere else. Users should adhere to the Ground Rules for use of TalkBank data.
INTRODUCTION
Joanne Steel
Emma Power
Davida Fromm
Brian MacWhinney
These materials are provided to students and clinicians who wish to improve their understanding of language-related problems accompanying traumatic brain injury (TBI). None of these materials should be copied or used anywhere outside of these web pages. In particular, none of the videos should be download or copied and placed anywhere else. Users should adhere to the Ground Rules for use of TalkBank data.
INTRODUCTION
Emma Power
Davida Fromm
Brian MacWhinney
These materials are provided to students and clinicians who wish to improve their understanding of language-related problems accompanying traumatic brain injury (TBI). None of these materials should be copied or used anywhere outside of these web pages. In particular, none of the videos should be download or copied and placed anywhere else. Users should adhere to the Ground Rules for use of TalkBank data.
INTRODUCTION
Davida Fromm
Brian MacWhinney
These materials are provided to students and clinicians who wish to improve their understanding of language-related problems accompanying traumatic brain injury (TBI). None of these materials should be copied or used anywhere outside of these web pages. In particular, none of the videos should be download or copied and placed anywhere else. Users should adhere to the Ground Rules for use of TalkBank data.
INTRODUCTION
Brian MacWhinney
These materials are provided to students and clinicians who wish to improve their understanding of language-related problems accompanying traumatic brain injury (TBI). None of these materials should be copied or used anywhere outside of these web pages. In particular, none of the videos should be download or copied and placed anywhere else. Users should adhere to the Ground Rules for use of TalkBank data.
INTRODUCTION
These materials are provided to students and clinicians who wish to improve their understanding of language-related problems accompanying traumatic brain injury (TBI). None of these materials should be copied or used anywhere outside of these web pages. In particular, none of the videos should be download or copied and placed anywhere else. Users should adhere to the Ground Rules for use of TalkBank data.
INTRODUCTION
What is TBIBank Grand Rounds?
TBIBank Grand Rounds is an online learning module that supports education about cognitive-communication disorders resulting from Traumatic Brain Injury (TBI). The primary aim is to enhance speech-language pathology assessment and treatment practices for the benefit of individuals with TBI.
Why was TBIBank Grand Rounds developed?
Psychosocial outcomes for individuals with severe TBI are extremely poor, with approximately 1 in every 2 individuals being unable to return to work (Corrigan et al., 2014) and approximately 1 in 3 reporting difficulties with personal relationships (Ponsford et al., 2014). To support these patients, speech-language pathologists (SLPs) require a thorough understanding of best-practice assessments and treatments for cognitive-communication disorders.
Evidence suggests that SLPs working with individuals who have had a TBI may lack knowledge and confidence in utilising best-practice assessment tools, such as discourse analyses (Bryant, Spencer, & Ferguson 2017). TBIBank Grand Rounds aims to promote best-practice in speech-language pathology by providing education on characteristics of discourse impairments, discourse analyses to complement assessment, and treatment approaches that target 'real-life' discourse-level communication activities. Supporting discourse-level communication has been shown to improve outcomes for individuals with TBI (Togher et al., 2013).Who is it designed for?
TBIBank Grand Rounds is designed for SLP educators, clinicians, and students to support various aspects of education such as teaching, clinical supervision, professional development, and in-services.
What is the scope of TBIBank Grand Rounds?
TBIBank Grand Rounds focuses on extended spoken discourse such as conversations, narratives, procedures and free speech, which is a primary area of difficulty for many individuals who have had a severe TBI (Elbourn et al., 2019). This is addressed within the context of holistic assessment and treatment for each case.
What content is included in TBIBank Grand Rounds?
TBI Grand Rounds provides case examples that showcase the range of spoken cognitive-communication disorders that can result from a severe TBI. The overarching framework of this learning resource is guided by the following questions:
- Cognitive-communication disorders
- Discourse profiles
- Variability across contexts
- Assessment of spoken discourse
- Management considerations
- Other communication disorders
- Recovery of spoken discourse
- Discourse treatments
How to use TBIBank Grand Rounds?
TBIBank Grand Rounds is designed to be used as a flexible teaching resource. The user may select a single video or segment to provide education on one particular cognitive-communication feature or alternatively, it can be used as a more complete teaching resource. We have also adapted the content and links into a PowerPoint presentation to assist with education and teaching (Please use the recommended citation below). There is also potential for clinicians to utilise TBIBank Grand Rounds as a self-guided professional development opportunity.
After reading this INTRODUCTION decide how you want to use the resource. If you choose to use this as a self-guided learning experience it is best to start with the pre-learning quiz and work your way through the modules sequentially. Each module follows a consistent structure beginning with relevant background followed by case studies then questions, suggested answers and, where relevant, additional resources.
Note: Names of individuals have been changed for confidentiality purposes. This resource is not intended to replace speech-language pathology coursework or clinical supervision but to support and enhance these processes.
Pre-learning Quiz
Note down your answers to the following questions so that you can revisit them at the end of the learning process. On a scale of 1-5 (1 = poor; 5 = excellent):
- How would you rate your understanding of the key similarities and differences between aphasia and a cognitive-communication disorder?
- How would you rate your knowledge of discourse profiles following TBI?
- How would you rate your understanding of the need to assess an individual in varied contexts?
- How would you rate your confidence with administering and analysing a discourse sample?
- How would you rate your knowledge of factors that might influence spoken discourse production?
- How would you rate your confidence with detecting other communicative comorbidities (apart from a cognitive-communication disorder) that may occur following a TBI (e.g., aphasia, dysarthria)?
- How would you rate your knowledge of recovery and prognosis of spoken discourse?
- How would you rate your understanding of treatment options for spoken discourse?
To cite this resource:
Elbourn, E., Togher, L., Steel, J., Power, E., Fromm, D., & MacWhinney, B. (2020, 10/08/2020). TBIBank Grand Rounds: Online education platform about cognitive-communication disorders resulting from Traumatic Brain Injury. https://tbi.talkbank.org/education/class-tbi/
Module 1: Cognitive-communication disorders
Cognitive communication disorders are a common consequence of traumatic brain injury (Ponsford, 2014; Gauthier 2018). By definition, a cognitive-communication disorder refers to any difficulty with communication (speaking, comprehension, reading, writing and social skills) that results from underlying cognitive impairment with attention, memory or executive functioning (College of Audiologists and Speech Language Pathologists of Ontario 2002, American Speech-Language-Hearing Association, 2004).
Some examples of how a cognitive-communication disorder can impact on communication include: difficulty taking turns in an interaction, difficulty staying on the topic of conversation, difficulty organising information in an orderly manner or difficulty interpreting non-verbal cues, such as facial expression.
Cognitive-communication disorders can affect work or academic performance (Douglas et al., 2016; Meulenbroek & Turkstra, 2016; Rietdijk et al., 2013) as well as everyday communication tasks such as having a conversation (Snow et al., 1998). Cognitive-communication competence can be influenced by many factors including emotional, physical and personal variables (MacDonald, 2017). The model pictured below helps to illustrate potential factors of cognitive-communication competence and how these factors relate to one another.
In this module, we demonstrate how cognitive-communication disorders can manifest in spoken discourse. The primary case, Liam (video 1a), is compared with a young male with no brain injury (video 1c) and an individual with aphasia (video 1b).
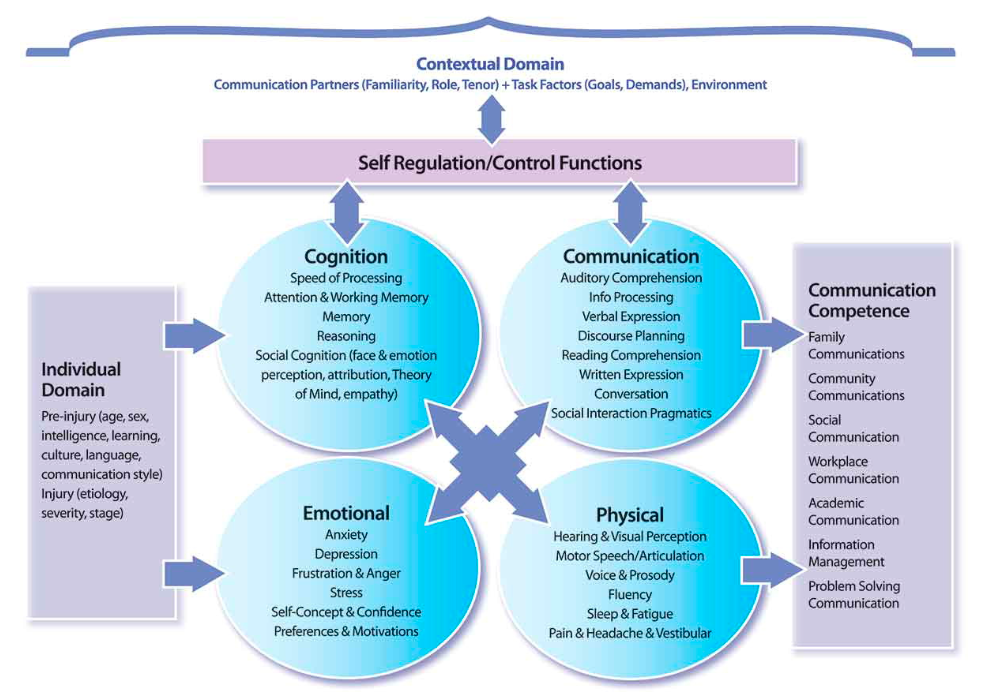
MacDonald, S. (2017). Introducing the model of cognitive-communication competence: A model to guide evidence-based communication interventions after brain injury. Brain Injury, 31, 13-14. Link to article
Case Studies
Case 1a is Liam, age 19, who sustained a severe traumatic brain injury from a motorcycle accident. He had no reported difficulties with hearing or vision. Pre-injury, Liam lived in the family home with his parents. His premorbid personality was described as a 'joker' and he was reported to have many friends. At the time of this video, Liam was 6 months post-injury. The video shows his retell of the Cinderella task from the TBIBank protocol. He indicated that he was familiar with the story. The La Trobe Communication Questionnaire (significant other report) was indicative of a social communication disorder.
Questions
- This short video highlights how communication can be affected by cognitive difficulties. What cognitive difficulties did you observe and how did these impact on Liam's communication?
Memory: Liam has difficulty recalling key components of the Cinderella story (e.g., attending the ball, meeting the prince and losing the glass slipper). With a memory prompt (e.g., Did Cinderella go to the ball and meet the prince?), he is able to continue with the story.
Attention: At the beginning of the story retell, Liam appears distractible (e.g., continually fiddling his hands and skin), which highlights his attention difficulties.
Processing speed: The long silence towards the end of the retell could reflect reduced processing speed as Liam is trying to remember the story and what he has already said about the story.
Executive functioning: Liam also has difficulty monitoring his retell of the story.
- Now compare this video with a person who has aphasia in video 1b and an individual with no acquired brain injury in video 1c. What is the difference in the language skills of these individuals?
Person with cognitive-communication disorder Person with aphasia Strengths Weaknesses Strengths Weaknesses Language skills are intact at word and sentence level.
No overt word retrieval difficulties.
Sentences are syntactically correct.
No morphological errors.
Macrostructure well organised.
Poor use of referents.
Macrostructure well organised. Difficulty with word-retrieval.
Presence of many semantic paraphasias.
Morphosyntactic errors are evident.
- In this module, we have selected the term 'cognitive-communication' to describe the communication changes that occur following a TBI. It is helpful to become familiar with the range of terminology that may be used in the context of TBI. Review the reading below and then consider the following question. In what contexts would you use the term cognitive-communication disorder versus another term and why?
Cognitive-communication disorder is the preferred term to describe the typical social communication difficulties that may arise after a TBI. This term reflects the interplay between the person's cognitive difficulties and their language functioning which is commonly affected following the diffuse brain damage that can occur with TBI. Another associated term used to describe common impairments following TBI includes disorders of social cognition and affect. These impairments relate to the difficulties a person with TBI may have, for example, with emotion perception and production, and theory of mind disorders (Cassel et al., 2019).
Additional Resources
Body, R., & Perkins, M. (2006). Terminology and methodology in the assessment of cognitive-linguistic disorders. Brain Impairment, 7(3), 212-222. doi:10.1375/brim.7.3.212
Cassel, A., McDonald, S., Kelly, M. & Togher, L. (2019). Learning from the minds of others: A review of social cognition treatments and their relevance to traumatic brain injury. Neuropsychological Rehabilitation, 29(1), 22-55, doi:1080/09602011.2016.1257435
Module 2: Discourse profiles
Background
Individuals with TBI typically have intact language skills at the level of words and sentences but significant challenges utilising discourse-level communication (Coelho et al., 1991b; Coelho et al., 2005a; Snow et al., 1995). Discourse refers to connected speech or a unit of language beyond a sentence (Halliday & Webster, 2009, Tannen, Hamilton, & Schiffrin, 2015) and can include both conversational and monologic discourse. The nature of discourse-level impairments can vary considerably among individuals with TBI (Coelho, Liles, & Duffy, 1991a; Covington & Duff 2016) and also across contexts (Snow et al., 1995; Togher 2000).
Common patterns can be observed in the monologues of individuals with TBI. Hartley and Jensen (1992) described three patterns of discourse impairments from a sample of 11 individuals with severe TBI during two narrative-based tasks. These patterns were: i) impoverished discourse, characterised by reduced productivity and content; ii) inefficient (or verbose) discourse, characterised by increased content and presence of verbal mazes; and iii) confused discourse, characterised by inaccurate content, confabulation, and ambiguous pronouns.
The previous learning module demonstrated how cognitive-communication disorders can manifest in spoken discourse. We identified that the individual produced insufficient information, had challenges organizing the characters and events of the story, and generated vague referents. The aim of Module 2 is to present three new cases to illustrate the variability that can occur with spoken discourse difficulties and highlight three common patterns of disorder: impoverished discourse, inefficient (or verbose) discourse and confused discourse. It is important to remember that there can still be individual variation within profiles (for example, an individual may predominantly demonstrate features consistent with an impoverished profile but may also have one or two features of the confused profile). The reader may also refer to Lê et al. (2011) for an example of an alternative approach to discourse profiling using the Story Goodness Index.
Case Studies
Videos 2a, 2b and 2c provide exemplars of three common discourse patterns. All three individuals had acquired a severe TBI three months earlier. Video 2a represents an impoverished example (Stimuli: TBIBank Protocol - free speech and important event), Video 2b illustrates an inefficient or verbose example (Stimuli: TBIBank Protocol - free speech recovery question), and Video 2c provides a confused example (Stimuli: TBIBank Protocol - free speech questions).
Questions
- What are the cognitive-linguistic features that are contributing to the description of the discourse in each of these cases?
Impoverished Inefficient (or verbose) Confused Short utterance length Excessive number of utterances produced in response to each question Response produced doesn't match the question that was asked Few utterances in response to each question Excessive detail provided on the topic Speaker produces utterance and pronouns that assume the listener has adequate presuppositional knowledge Non-specific vocabulary - 'all the courses', 'stuff like that', 'normal stuff' Fails to bring the topic to a close at an appropriate point Lack of coherence between utterances and rapid topic changes - Identify at least one discourse analysis that you think would be helpful for each of these cases?
Impoverished Inefficient (or verbose) Confused Total communication units in discourse (Hartley & Jensen, 1992) Percent of syllables in mazes (Hartley & Jensen, 1992) Cohesion analysis (Problems of reference) (Hartley & Jensen, 1992) Narrative tasks - Story completeness score (Power et al., 2020) Narrative tasks - Story grammar score (Power et al., 2020) Narrative tasks - Percentage of correct story grammar elements (Steel et al., 2017) or coherence analysis (Van Leer & Turkstra, 1999) - Video 2a is almost in direct contrast to video 2b. How might this influence your potential goals and approach to therapy?
A potential goal for 2a may be the production of an increased number of words and T-units in spoken discourse; whereas for 2b, the goal may be focused on decreasing the number of T-units produced in spoken discourse. Utilising video or audio feedback to support improved awareness and insight into these challenges might be a useful approach for both of these individuals.
Module 3: Variability across contexts
Background
The sociolinguistic framework has been utilised to explore the discourse skills of individuals with TBI across a variety of situations and contextual variables (Armstrong, 2005; Togher, 2001). This approach to discourse has revealed that the communicative performance of individuals with TBI can be significantly impacted by context and the genre of communication (Snow & Douglas, 2000; Togher, 2000).
Individuals with TBI have been shown to perform differently when the purpose of communication is varied. For example, one study compared seven individuals with TBI and matched controls across two tasks; an information-giving task (community education session) and an information-requesting task (asking questions about the project) (Togher 2000). It was found that when placed in an information-giving role, individuals with TBI provided similar information to controls which was in contrast to the information requesting role (Togher, 2000). Another study, examining procedural discourse in 26 individuals with TBI, found no significant differences in the main outcome measure when compared to controls (Snow, Douglas, & Ponsford, 1997). This was discussed in the context of the procedural genre as a well-learned and familiar sequence that draws upon relatively spared procedural memory (Snow et al., 1997). These studies highlight the importance of evaluating varied spoken discourse genres. The TBIBank protocol (Discussed further in Module 4) is a useful tool for evaluating varied spoken discourse genres.
Also, communication partners are an integral component of context and have been shown to influence the communicative performance of individuals with TBI (Tu et al. 2011). Communication partners can employ strategies to facilitate or hinder communicative performance of individuals with TBI (Togher et al., 1997). Furthermore, positive strategies can be developed through communication partner training and can improve everyday conversations of individuals with TBI (Rietdijk, 2013; Togher et al., 2013 ). Hence, examining communication partner behaviour as part of the context of communication and how the individual with TBI responds to these behaviours can be invaluable for assessment.
In this module we illustrate how different contexts and genres can impact on spoken discourse. Videos 3a, 3b, 3c, and 3d show Liam from Module 1 firstly, participating in a conversation with his mother (video 3a). Next, he responds to the free speech questions from the TBIBank protocol (video 3b). He then produces a range of narrative-based tasks (video 3c) and the final spoken discourse task is a procedure (video 3d), again from the TBIBank Protocol.
Pictures used in the picture description videos:
Window
Umbrella

Cat in Tree
Case Studies
Questions
- Liam's cognitive-communication skills were highlighted in Module 1. What new information did you gain about Liam's communication from the additional context and genres shown here in Module 3? What do you perceive as Liam's greatest cognitive-communication difficulties and strengths?
- Drawing upon your observations of the different genres, what direct and indirect supports could be helpful to support Liam with his spoken discourse?
| Conversation | Free Speech Tasks | Picture Description & Narratives | Procedure |
|---|---|---|---|
| Pragmatic and social communication strengths - e.g., adequate turn-taking skills and good eye contact Difficulties -- e.g., topic initiation and inappropriate social behaviour both verbally and non-verbally | Provides insight into Liam's awareness of his cognitive-communication difficulties and potential lack of motivation for therapy | Compared to the Cinderella narrative in Module 1, these narratives are more organised and complete (with the visual prompts provided by the narrative and picture description tasks) | Fairly well organised but shows some subtle memory difficulties |
| Conversation | Free Speech Tasks | Picture Description & Narratives | Procedure |
|---|---|---|---|
| Training communication partners in how to direct Liam to initiate appropriate conversation topics could be helpful | Improving self-awareness of his cognitive-communication difficulties could be a helpful starting point for more direct rehabilitation of spoken discourse. | Visual supports such as photos and sequencing, 'wh' questions to guide narrative production and generic structures to organise spoken discourse. | Drawing on Liam's relatively intact procedural memory skills could be another useful strategy. |
Module 4. Assessment of spoken discourse
Background
A range of tools can be used to support assessment of cognitive-communication disorders. In 2005, the Academy of Neurologic Communication Sciences and Disorders (ANCDS) published an evidence-based review of both standardised (Turkstra et al., 2005) and non-standardised measures (Coelho et al., 2005) for assessing cognitive-communication disorders. Assessment for social communication is addressed specifically in Steel and Togher (2019) as well as Sohlberg et al. (2019). The reader is encouraged to consult these documents for an overview of cognitive-communication assessment.
This module focuses specifically on assessment of spoken discourse as part of a complete cognitive-communication assessment. Assessments for spoken discourse are typically categorised as either monologic or dialogic (conversational). The TBIBank Protocol (TBIBank - see Protocol List and Protocol Instructions links) includes some of the most commonly elicited monologic discourse tasks including free speech, recount, picture description, narrative and procedural genres. As demonstrated in Module 3, assessment can be strengthened by including elicitation of both a conversation sample and a range of monologic discourse genres.
Once a discourse sample has been obtained, the next step involves analysing the discourse sample. There are a wide range of discourse analysis options available and it can be challenging to know which analysis will be most informative for each person. Togher (2001) offers a useful overview of discourse analyses, derived from the Systemic Functional Linguistic framework, that have been shown to capture complexity of communication difficulties in dialogic and conversational samples (Togher, 2001). Alternatively, synthesised evidence for selection of monologic discourse analyses are presented by Coelho et al. (2005) with the conclusion that analyses of "productivity and efficiency of verbal output, content accuracy and organisation, story grammar and coherence" (p. 230) have the most evidence for capturing spoken discourse challenges. The table below outlines some suggested discourse analyses for each component of the TBIBank Protocol.
| TBIBank Protocol Task | Genre | Potential Analyses* |
|---|---|---|
| Brain Injury Story & Coping | Free Speech | Productivity |
| Important Event | Recount | Efficiency |
| Broken Window | Picture description/Narrative | Story grammar analysis |
| Cat Rescue | Picture description/Narrative | Content accuracy |
| Cinderella | Narrative retell | Main concept analysis |
| Sandwich | Procedure | Coherence |
| Conversation | Conversation | Exchange structure analysis |
Case Studies
There are no case studies for this module. Instead, we would encourage you to complete the following tasks to build your clinical skills:
- Download the TBIBank protocol and the stimuli materials and practice administering the questions. You might like to involve another person such as a peer.
- Select one or two analyses and practice applying the analysis with one of the samples provided on this site.
Questions
- Reflect on your experience of administering the protocol. What parts did you find easiest or hardest to administer?
It is recommended that you follow the standardised administration of the TBIBank protocol. It can take some practise to; deliver the questions in a natural manner, to know when to use the troubleshooting questions or to know how to provide encouragement and feedback to the person completing the task.
- Reflect on your experience of completing the discourse analysis. What did you learn from completing this task?
We hope that you have learned about the value of completing a discourse analysis from this task. Although it may take time initially to learn the analysis, you can gain valuable information about a person's cognitive-communication skills that simply can't be captured from other language-based assessments.
Module 5: Management considerations
Background
Cognitive-communication disorders can also be affected by the additional emotional and behavioural sequalae resulting from traumatic brain damage. Some of the common and persisting consequences of TBI include depression, emotional lability, self-awareness deficits, lack of motivation, fatigue, confabulation and pain (Bajo et al., 2017; Cantor et al. 2012; Fleming & Strong, 1999; Irvine & Clark, 2018; Morton & Wehman 1995; Ponsford et al., 2014; Sloan, Brown, & Pentland, 1992). The presence of these additional consequences is highly individual, and it is important to note that this is not an exhaustive list of sequalae. Nevertheless, these common sequalae that result from TBI can play a role in facilitating and/or hindering cognitive-communication performance. Addressing these sequalae requires a team-based approach to management including medical, psychological, and other health professionals. In this module, we highlight how the outlined sequalae can impact spoken discourse performance, and we consider implications for management.
The first factor that is explored in this module is the presence of depression (video 5a), that is, a persistent feeling of sadness and loss of interest in enjoyable activities which also impacts on daily functioning (Seel, Macciocchi, & Kreutzer, 2010). Mental health condition, such as depression, are common following TBI and can potentially impact interpersonal communication skills and the quality of social relationships (Morton & Wehman, 1995; Tse & Bond 2004; Williams & Evans 2003).
Emotional lability, referring to rapid and exaggerated changes in feelings and emotions is another common experience for individuals with a TBI (video 5b). Emotional lability is caused by damage to parts of the brain that control emotions and behaviour. Emotional lability can potentially be distressing and embarrassing for individuals and their communication partners (Sloan et al., 1992).
Deficits with self-awareness or a lack of insight occurs when an individual is unaware of the deficits resulting from their brain injury (video 5c). Self-awareness deficits commonly result from injuries to the frontal lobes. These deficits can lead to poor motivation, lack of cooperation and irritability as the individual is unable to understand the need for rehabilitation (video 5d) (Fleming & Strong 1999; Ownsworth & Clare 2006).
Another factor highlighted in this module is fatigue, whereby a person experiences significant physical or mental exhaustion from everyday activities such as having a conversation (video 5e). Fatigue can also be related to sleep disruption (Ponsford et al., 2012; Wiseman-Hakes et al., 2009). Persistent fatigue can be highly debilitating, affecting a person's ability to lead a normal life (Cantor et al., 2012). Fatigue can also impact on speech pathology assessment and treatment.
Confabulation can be particularly common in the early stages after TBI and it is a condition where an individual generates false memories, perhaps reporting an event that never occurred (Bajo et al., 2017). Confabulation is unintentional and differs from lying as the individual is conveying information that they believe to be true (Hirstein, 2009). It has been suggested that confabulation is caused by executive control deficit and evaluation deficit (Metcalf et al., 2007, 2010). The mechanism may be related to impairment of both ability to retrieve and select the correct memory of what to say, and to evaluate how likely or relevant the retrieved material is (Metcalf et al., 2007, 2010). Confabulation has the potential to inadvertently cause harm, for example, if information around finances or medical conditions is not verified for accuracy. An example of confabulation is provided in transcript 5f.
On a final note, pain such as headaches (Irvine & Clark, 2018) and the potential impact of medications (Merino et al., 2019) need to be considered as part of a holistic client management plan.
Case Studies
Case background: Paul was a 27-year-old man, who was bilingual with English as his second language. He was proficient in English, having worked in Australia for several years as a professional sportsperson. He had a severe TBI (PTA duration 24 days) from a sports accident. After his injury he had visual difficulties and severe headaches, that persisted at three months after PTA emergence. He had not been able to return to work. During PTA Paul was confused and had difficulty understanding why he was in hospital, and he did not remember details from day to day. He was cooperative in sessions although perseverative about going home, and he occasionally confabulated about his situation.
This first transcript (transcript 5f) was produced when Paul was in PTA, scoring 8/12. The transcript is a short conversation between Paul and a speech-language pathologist (SP). His wife and baby were frequent visitors to hospital. The second transcript (transcript 5g) shows Paul describing the broken window picture prior to PTA emergence (11/12) and 3 months post-emergence. At the follow up session, Paul reported having a bad headache, although still consented to the assessment session. Note: Ongoing measurement of PTA begins once the person emerges from coma and is able to participate in daily testing. In Australia, the most commonly used measure is the Westmead Post-Traumatic Amnesia Scale (WPTAS) (Shores et al., 2008). Daily testing commences once the person is capable of responding. The WPTAS comprises seven orientation questions and five memory questions, and the person is tested until able to correctly answer 12/12 questions for three days in a row (or on the first day scoring 12/12 after 28 days in PTA).
Transcript 5f
SP Who is in your family?
P I have children, my wife.
SP So what other children do you have?
P I have five children.
SP Ah, so they're still in [country] are they?
P Yes.
SP Who are they staying with?
P Some are married, some, you know, with my family, that's it.
Transcript 5g
Paul: Broken window story, PTA 11/12, 34 seconds
P Playing with football, air conditioned or a heater, and (06) that's pretty all.
SP Can you tell me anything else?
SP Just try and tell the story with a beginning, a middle and an end if you can.
P Ah he's sitting on couch, playing football kind of.
P Tried to throw on the window and he's grabbing back.
P He's hold on the window, and tried to give it back, football thing.
P That's the best I can come I think.
P Mm, first one kicking the ball (03) mm. (04).
P Mm, I can't recognise the second one, air conditioning or television. (11)
P I see third one sitting on the chair, I mean on the lounge (um), got next ball probably coming to him. (07)
P And fourth one, got the ball in the hand, and he maybe thinking to throwing out.
Questions
- Video 5a: Watch the video of this 40-year-old man who was 9 months post-injury at the time of recording. What do you notice about this person's facial expression and tone of voice? Who might you collaborate with to support this person?
You probably noticed the flat affect and monotone voice quality of this individual. A referral to a clinical psychologist would be indicated if these features persist.
- Video 5b: This next video shows the same person at 12 months post-injury. Note any differences that you observe from the previous video. The person laughs about a potentially upsetting story. How might this be perceived in a social context? How could this pragmatic behaviour potentially be managed?
This person's emotional response is misaligned with the story. This could be perceived as insensitive. Communication partners might benefit from information about the effects of brain damage on emotional control and strategies to support these scenarios such as not responding to the exaggerated emotion and redirecting communication.
- Video 5c: This clip shows a 53-year-old man responding to the recovery story question from the TBI Bank Protocol. How would you describe his level of awareness/insight into his cognitive-communication difficulties?
The person in this clip acknowledges challenges with his communication. However, you will note that he is unable to monitor and change these behaviours as he is talking.
- Video 5d: In this video we revisit the case Liam to explore his responses to the free speech tasks. Liam doesn't appear to be highly motivated while participating in this task. How do you think this might be reflected in his other rehabilitation activities?
Liam did not acknowledge any significant changes in his communication skills. Consequently, Liam struggles to understand why he needs rehabilitation, and this affects his engagement with rehabilitation tasks. Helping Liam to build insight into his communication difficulties would be a useful starting point for rehabilitation.
- Video 5e: In this segment, we revisit the first video of Liam producing the Cinderella narrative. In this video, he shows objective signs of fatigue such as yawning on multiple occasions. Reflect on your own experiences of feeling fatigued. How did this impact on your communication skills?
Varied responses. Fatigue can be highly debilitating. Managing fatigue as part of a team (e.g., with the use of structured rest periods) can be an important strategy in promoting positive communication.
- Transcript 5f: There is evidence of confabulation in this sample. How could you support the individual and family with confabulatory communication?
Confabulation can be very confronting. It can be helpful to provide communication partners with education around confabulation (e.g., the behavioural changes stem from the injury and are not the 'fault' of the person) and ways of approaching confabulation such as providing clear, accurate information and avoiding arguing with the person.
- Transcript 5g: What effect might Paul's headache and vision difficulties have on his production of discourse samples? How could you address the impact of motivation level and effort on the sample when you are eliciting discourse?
Paul appears to have difficulty perceiving the stimuli in this task and doesn't appear to be attending well to the task. This sample also highlights the importance of obtaining qualitative data on the condition of the person on the day of assessment.
Module 6: Other communication disorders
Background
Cognitive-communication disorders are highly prevalent following TBI (Elbourn et al., 2019). However, there are a range of other communicative comorbidities that can result from a TBI in addition to a cognitive-communication disorder (Sarno, 1980). Clinicians need to be able to readily screen for these disorders and conduct further assessment if difficulties are identified.
Aphasia, an impairment of language, is a condition where an individual has difficulty understanding and using the symbols of language. The AphasiaBank Grand Rounds details the various types of aphasia that can result from left hemisphere stroke. The aphasia sample in this module, highlights an individual with aphasia in addition to a cognitive-communication disorder as a result of a TBI. The combined language disorder and cognitive-communication disorder can be particularly challenging for clinical assessment and treatment. Word-finding difficulty, paraphasias and comprehension difficulties may be a result of left hemisphere damage, or they may be a result of more generalised cognitive impairments such as memory, slowed processing and attention (Kerr, 1995). The incidence of aphasia following TBI is highly variable due to this complex interplay between cognition and language. A recent study identified frank aphasia in 16% of a cohort at 3-6 months post-TBI and presents a potentially new approach to utilising the WAB-R (Kertesz, 2012) for diagnosis of aphasia following TBI (Elbourn, Kenny, Power, Honan, et al., 2019). The INCOG: cognitive-communication guidelines (Togher et al., 2014) and the ANCDS standardised assessment guidelines (Turkstra et al., 2005) offer useful frameworks for approaching clinical assessment of aphasia in the context of TBI and a cognitive-communication disorder.
Dysarthria refers to a motor speech disorder in which the muscles used for speech are weak or poorly controlled. Speech is commonly slurred, slow and effortful, with poor articulation of sounds and, in the case of TBI, is characterised by marked prosodic changes (Wang et al., 2005). Dysarthria can impact on quality of life, social connection and employment (Guo & Togher, 2008). Dysarthria may also influence how an individual is treated by others and it commonly co-exists with other physical disability (Walshe & Miller, 2011).
Apraxia of speech is a motor planning or programming disorder affecting speech production. Individuals with apraxia of speech have adequate strength and coordination of the speech muscles but have difficulty saying words correctly and consistently. Signs of apraxia of speech that have been reported following TBI include "articulatory groping, sound distortions, substitutions, additions and exchanges, poor transitions between syllables and words, reduced rate of speech, difficulty with sequencing of syllables and phonemes, and difficulty initiating speech" (Friedman et al., 2010, p.19).
Voice disorders can also result from a TBI and are characterised by a voice quality, pitch or loudness that is either abnormal or insufficient to meet the persons daily needs. Voice disorders resulting from TBI are considered organic neurogenic voice, resulting from problems with the parts of the nervous system that control the larynx, or mechanical (e.g., resulting from intubation). Voice disorders have been reported in up to 58% of individuals with a communication disorder post TBI (Norman et al., 2013). Individuals with TBI are reported to have incomplete laryngeal valving, resulting in perceptual ratings of breathiness, with correlations in acoustic measures, such as abnormal amplitude perturbation and noise-to-harmonic ratio (McHenry, 2000).
Social or pragmatic communication deficits include difficulty using verbal or nonverbal language for social purposes. Social communication disorders can result from impairments in any or all component areas of speech, language and cognitive-communication (Steel & Togher, 2019) and can manifest in a variety of ways. The two case examples that are provided in this module focus on impairments of social communication characterised by elevated dysfluency and impacted speech rate, which may also be related to mild dysarthria (Wang et al., 2005).
Case Studies
Questions
- Video 6a shows a 56-year-old woman who presents with aphasia in addition to a cognitive communication disorder as a result of a motor vehicle accident. In this video, she is producing the cat story retell and the procedural discourse tasks. Her Aphasia Quotient score on the Western Aphasia Battery-Revised (WAB-R; Kertesz, 2012) was 84, with predominant difficulties with naming and word-retrieval and relative strengths with auditory comprehension, automatic naming and repetition, consistent with mild anomic aphasia. Her performance on the Boston Naming Test (Kaplan, Goodglass, & Weintraub, 2001) was 10/60. What features of her spoken discourse are more consistent with aphasia vs cognitive-communication disorder?
The features that are reflective of aphasia in this sample include the high frequency of unrelated semantic paraphasia and the presence of perseveration. Paraphasias that occur in the absence of aphasia are typically related semantic paraphasias, that is, the error word is closely related to the target word. Features of the cognitive-communication disorder can be difficult to disentangle from the aphasia however there is evidence of executive functioning difficulty. For example, the person appears to have difficulty reflecting on her performance and approaches to procedural discourse task from an egocentric point of view.
- Video 6b: This video shows a 42-year-old man who presents with a severe dysarthria in addition to a cognitive-communication disorder. Mechanism of injury was a fall and crush. In this video he is completing the important event and the broken window discourse tasks. The Frenchay Dysarthria Assessment-2 (Enderby & Palmer, 2008) highlighted most difficulty with reflexes, lip, larynx and tongue movements, impacting significantly on intelligibility. His respiration and palatal movements were relatively unaffected. What features of dysarthria do you observe in the video? How does the dysarthria impact the fluency of his spoken discourse?
This individual presents with slow, effortful and imprecise articulation. There is increased phoneme duration and challenges with phoneme transitions which leads to reduced fluency and intelligibility of spoken discourse.
- Video 6c shows a 19-year-old man who presents with Apraxia of Speech in addition to aphasia and a cognitive communication disorder as a result of a motor vehicle accident. His WAB-R Aphasia Quotient was 39. What signs do you observe in this video that would suggest further assessment of apraxia is required?
In this video, you might observe articulatory groping and difficulty initiating speech, sound substitutions, additions and exchanges, poor transitions between syllables and words and difficulty with sequencing of syllables and phonemes. This person would benefit from further assessment with a tool such as the Apraxia Battery for Adults-2 (Dabul, 2000).
- Video 6d is a 16-year-old woman who presents with a voice disorder post-TBI. The person discusses her voice disorder and the relationship to her length of intubation. What would be an important step in managing her voice disorder?
Considerations for management of this individual's voice disorder should include a referral to a laryngologist and/or and ear, nose and throat specialist for visualisation of the vocal mechanism as well as further assessment of voice with a range of appropriate perceptual and acoustic measures.
- Video 6e shows a 45-year-old man who presents with dysfluency as a result of his TBI. What would be a useful measure for capturing his dysfluency? How might fluency be addressed?
Further assessment of the nature of this individual's dysfluency would be valuable. The reader might be interested to read the paper by Penttilä, Korpijaakko-Huuhka, and Kent (2019) which details the nature and categorisation of dysfluency following TBI. Delayed auditory feedback is a potential treatment area that has also been explored in the context of dysfluency following TBI (Van Borsel, Drummond, & de Britto Pereira, 2010).
- Video 6f is a 22-year-old man who demonstrates a very fast speech rate in combination with a dysarthria and a cognitive-communication disorder. How might you approach rehabilitation differently for this individual in comparison with the man with dysarthria in video 6a?
Compared to video 6a, the person in this video appears to have reduced awareness of his dysarthria as he doesn't appear to make any compensations for his dysarthria. A potential approach for this individual might be to develop improved awareness of his dysarthria and encourage reduced speech rate to support improved intelligibility.
Module 7: Recovery of spoken discourse
Background
The overall goal of rehabilitation following TBI is to optimise recovery and outcomes for the person (Elbourn et al., 2016). Recovery of spoken discourse following a severe TBI is strongly associated with important everyday psychosocial outcomes relating to work, relationships, and independence (Elbourn, Kenny, Power, & Togher, 2019).
During early recovery and the period of PTA, it is feasible to assess cognitive-communication skills through spoken discourse (Steel et al., 2017). Furthermore, despite some transient changes in cognition and behaviour, assessment during PTA can support prediction of ongoing cognitive-communication skills (Steel et al., 2017) and also contribute information about PTA resolution (Sherer et al., 2020). Other predictive factors relating to discourse recovery during the subacute stage include the presence of aphasia, PTA duration, pre-injury level of education and age (Elbourn et al., 2018; Elbourn, Kenny, Power, & Togher, 2019). Individual motivation and social support should also be considered when predicting patient outcomes and planning services.
Many individuals with TBI will show recovery of spoken discourse skills within the first year following their injury but the skills may not return to pre-injury levels within this timeframe (Elbourn et al., 2017) and ongoing rehabilitation is often required. A common misconception is that individuals with TBI may experience a plateau of recovery after the initial 3-6 months post-injury, however we now know that improvements in spoken discourse can occur up to 12 months following injury (Elbourn et al., 2018) and possibly beyond (Snow et al., 1999). In fact, six months post-injury is a beneficial time for assessment, education, and service planning (Elbourn, Kenny, Power, & Togher, 2019).
Case Studies
Case background: Sam was a male in his 30s, who had worked as a professional before the accident, and had a high level of language proficiency. His PTA duration was 3 weeks. After the injury, he returned to part-time work, with persisting memory, vision and concentration problems (self-reported and on neuropsychological testing). During PTA, Sam's language skills were WNL on standardised testing, but he scored well below expected level on verbal fluency. These features had resolved at follow up.
Transcript 7e
Sam: Broken window story: During PTA (11/12)
P Alright, so you've got, young kid has kicked a ball, (uh) straight through somebody's window.
P (Um) the person who owns the window was sitting just inside as the ball came in, looked at the ball and went oh my goodness.
P Looks like it knocked the lamp over as well, (um).
P So he immediately picked up the ball and looked out to see who might have kicked it in.
P But of course whoever kicked it in had long vanished.
Sam: Broken window story: Three months after PTA emergence
P Okay so the next picture is (um), a boy, playing with his soccer ball, possibly in a field.
P He gives the ball a good kick.
P And it goes straight through a window, (um) shattering (the gl-) the glass.
P (Um), it goes through the window.
P And there is a man sitting inside on his chair.
P As the ball comes in, it knocks over his lamp, which probably gets his attention.
P And the last picture seems to be the man holding the soccer ball and looking out the window I suppose to see who might have caused the accident.
Questions
- Video 7a shows a 22-year-old woman at 3 months post-injury producing a retell of the Cinderella narrative. Video 7b shows the same woman again at 12 months post-injury completing the same retell task. What changes do you observe in her production of the Cinderella narrative from 3 months to 12 months?
There are clear improvements in the discourse between initial and follow-up for this individual. The initial narrative could be described as brief, vague and disorganised. In the follow-up video the content is much more detailed and organised, and she uses more specific language.
- Video 7c is a 29-year-old man at 3 months post-injury producing a retell of the Cinderella narrative. Video 7d shows the same man again at 12 months post-injury completing the same retell task. How would you describe the difference between his initial production and the follow-up?
This person has minimal improvement in his production from the initial assessment to follow-up. Challenges with idea generation, memory, specific terms/vocabulary, absence of main concepts and slow speech rate are evident in both samples. The main concept score was initially 5 and at the second time point was 7. However, this is not considered a clinically reliable change (Elbourn, Kenny, Power, Honan, et al., 2019). Qualitatively you might observe some subtle improvements such as more specificity in his vocabulary and a faster speech rate.
- Transcript 7e shows changes in the discourse of Sam from the period of PTA and at 3 months post-injury. How would you characterise changes in Sam's narrative production before and after PTA resolution?
Sam's production at the follow-up is relatively more detailed and better organised than the initial assessment. Whilst Sam's grammar is intact at initial assessment, he utilises more complex grammatical structures in the follow-up production. There is also more detail in the narrative of the second sample.
Module 8: Discourse treatments
Background
Recent evidence-based reviews of cognitive-communication interventions support person-centred approaches to treatment for individuals with TBI (Meulenbroek et al., 2019; Togher et al., 2014). Person-centred approaches ensure that rehabilitation is tailored to the individual's needs, goals and skills (Togher et al., 2014).
Some of the key principles that support effective rehabilitation include consideration of premorbid communication status as well as contextual based learning to facilitate generalisation of skills (Meulenbroek et al., 2019; Togher et al., 2014). Another principle is the inclusion of instructional strategies that offer cognitive support such as errorless learning, awareness training and metacognitive approaches (Finch et al., 2017).
Modest evidence exists for the effectiveness of communication partner training (Behn et al., 2012; Rietdijk et al., 2020a, 2020b; Togher et al., 2004; Togher et al., 2013) and social communication groups (Dahlberg et al., 2007; Keegan et al., 2019; Parola et al., 2019) that integrate the aforementioned principles. Identifying the active ingredients of treatment for cognitive-communication disorders and spoken discourse disorders remains largely unknown (Coelho, 2007; Meulenbroek et al., 2019). However, there are some promising avenues for targeted treatments such as the communication-specific coping intervention (CommCope-I) (Douglas et al., 2019), discourse processing treatment (Kintz et al., 2018) and work-related communication training for employment readiness (WoRCTER) (Meulenbroek & Cherney, 2018).
Additionally, where appropriate, training in the use of assistive technology and treatment for aphasia is recommended (Togher et al., 2014).
Case Studies
Review the case of Liam, featured in Modules 1, 3 and 5.
Questions
- What might be some potential goals that could be targeted as part of a communication partner training including Liam and his mother?
Goals could include identifying communication situations which are important to Liam, such as meeting his friends socially. Targeted skills could include verbal aspects of communication such as topic initiation and maintenance, non-verbal aspects of communication such as body proximity or cognitive-based skills such as memory and recall of conversations.
- Explore and discuss some potential instructional strategies that might be useful for Liam's case?
Treatment could focus on improving his self-monitoring skills with the use of rating scales and video feedback, improving the length of time he concentrates during a social activity, and using metacognitive strategy instruction to develop goal-setting, self-regulation, and task analysis for functional communication activities.
- How might a social communication group be beneficial for Liam?
A social communication group might provide a real opportunity for Liam to practise his social skills. It may also offer opportunity to develop self-awareness of his cognitive-communication skills.
Glossary
| Cognitive-communication disorder | Any difficulty with communication (speaking, comprehension, reading, writing and social skills) that results from underlying cognitive impairment with attention, memory or executive functioning (American Speech-Language-Hearing Association, 2004; College of Audiologists and Speech Language Pathologists of Ontario, 2002). | |
| Confabulation | A condition where an individual generates false memories, perhaps reporting an event that never occurred (Bajo et al., 2017). Confabulation is unintentional and differs from lying as the individual is conveying information that they believe to be true (Hirstein, 2009). | |
| Discourse | Discourse refers to connected speech or a unit of language beyond a sentence (Halliday & Webster, 2009; Tannen et al., 2015). | |
| Executive Functions | Cognitive skills that enable a person to form goals, plan goals, execute the plan and evaluate performance (Jurado & Rosselli, 2007). | |
| Metacognitive | Otherwise known as 'thinking about thinking'. The ability to plan, monitor and evaluate thinking processes. | |
| Post-traumatic amnesia | Post-traumatic amnesia is a transient stage early in the recovery process after TBI, characterised by confusion, memory and orientation impairments, and behavioural disturbances (Levin et al., 1979). This confusional state may last from minutes to several months. Although progression through PTA is gradual, there can be "islands" of memory and the condition is best described as fluctuating. | |
| Self-awareness deficit | Also referred to as a lack of insight, a condition that occurs when an individual is unaware of the deficits resulting from their brain injury. Self-awareness deficits commonly result from injuries to the frontal lobes. | |
| Social cognition disorder | These impairments relate to the difficulties a person with TBI may have, for example, with emotion perception and production, and theory of mind disorders (Cassel et al., 2019). |
References
American Speech-Language-Hearing Association (2004). Preferred Practice Guidelines for the Profession of Speech-Language Pathology. https://www.asha.org/policy/ (last accessed).
Armstrong, E. (2005). Language disorder: A functional linguistic perspective. Clinical Linguistics and Phonetics, 19, 137-53.
Bajo, A., Fleminger, S., Metcalfe C., & Kopelman, M. D. (2017). Confabulation: What is associated with its rise and fall? A study in brain injury. Cortex, 87, 31-43.
Behn, N., Togher, L., Power, E., & Heard, R. (2012). Evaluating communication training for paid carers of people with traumatic brain injury, Brain Injury, 26(13-14), 1702-1715. doi:10.3109/02699052.2012.722258
Bryant, L., Spencer, E., & Ferguson, A. (2017). Clinical use of linguistic discourse analysis for the assessment of language in aphasia. Aphasiology, 31, 1105-1126. doi:10.1080/02687038.2016.1239013
Cantor, J. B., Bushnik, T., Cicerone, K., Dijkers, M. P., Gordon, W., Hammond, F. M., Kolakowsky-Hayner, S. A., Lequerica, A., Nguyen M., & Spielman, L. A. (2012). Insomnia, fatigue, and sleepiness in the first 2 years after traumatic brain injury: An NIDRR TBI model system module study. The Journal of Head Trauma Rehabilitation, 27, E1-E14.
Cassel, A., McDonald, S., Kelly, M., & Togher, L. (2019). Learning from the minds of others: A review of social cognition treatments and their relevance to traumatic brain injury. Neuropsychological Rehabilitation, 29(1), 22-55.
Coelho, C., Liles, B. Z., & Duffy, R. J. (1991a). Discourse analyses with closed head injured adults: evidence for differing patterns of deficits. Archives of Physical Medicine and Rehabilitation, 72, 465-8.
Coelho, C. (1991b). The use of discourse analyses for the evaluation of higher level traumatically brain-injured adults. Brain Injury, 5, 381-392.
Coelho, C., Ylvisaker, M., & Turkstra, L. S. (2005a). Nonstandardized assessment approaches for individuals with traumatic brain injuries. Seminars in Speech and Language, 26, 223-41.
Coelho, C., Ylvisaker, M., & Turkstra,L. S. (2005b). Nonstandardized assessment approaches for individuals with traumatic brain injuries. Seminars in Speech & Language, 26, 223-41.
College of Audiologists and Speech Language Pathologists of Ontario. (2002). Preferred practice guideline for cognitive-communication disorders.
Corrigan, J. D., J. P. Cuthbert, C. Harrison-Felix, G. G. Whiteneck, J. Bell, A. C. Miller, V., Coronado, G., & Pretz, C. R. (2014). US population estimates of health and social outcomes 5 years after rehabilitation for traumatic brain injury. Journal of Head Trauma Rehabilitation, 29, E1-9.
Covington, N., & Duff, M. (2016). Intact reported speech use in traumatic brain injury: How to think about 'intact' performance in the context of heterogeneity. Journal of Interactional Research in Communication Disorders, 7, 79.
Dabul, B. L. (2000). Apraxia Battery for Adults. Texas:ProEd.
Dahlberg, C. A., Cusick, C. P., Hawley, L. A., Newman, J. K., Morey, C. E., Harrison-Felix, C. L., & Whiteneck, G. G. (2007). Treatment efficacy of social communication skills training after traumatic brain injury: a randomized treatment and deferred treatment controlled trial. Archives of Physical Medicine and Rehabilitation, 88(12), 1561-1573.
Douglas, J., M., Bracy, C. A., & Snow, P. C. (2016). Return to work and social communication ability following severe traumatic brain injury. Journal of Speech, Language, and Hearing Research, 59, 511-520.
Douglas, J. M., Knox, L., De Maio, C., Bridge, H., Drummond, M., & Whiteoak, J. (2019). Effectiveness of communication-specific coping intervention for adults with traumatic brain injury: Preliminary results. Neuropsychological Rehabilitation, 29(1), 73-91.
Douglas, J. M., O'Flaherty, C. A., & Snow, P. C. (2000). Measuring perception of communicative ability: the development and evaluation of the La Trobe communication questionnaire. Aphasiology, 14(3), 251-268.
Elbourn, E., Kenny, B., Power, E., Honan, C., McDonald, S., Tate, R., Holland, A., Macwhinney, B., & Togher, L. (2019). Discourse recovery after severe traumatic brain injury: exploring the first year. Brain Injury, 33, 143-159.
Elbourn, E., Kenny, B., Power, E., Honan, C., & Togher, L. (2018). Discourse recovery after severe traumatic brain injury: Exploring the first year. Brain Injury. [Under review]
Elbourn, E., Kenny, B., Power, E., & Togher, L. (2019). Psychosocial outcomes of severe traumatic brain injury in relation to discourse recovery: a longitudinal study up to 1 year post-injury. American Journal of Speech-Language Pathology, 28(4), 1463-1478.
Elbourn, E., Togher, L., Kenny, B., & Power, E. (2016). Strengthening the quality of longitudinal research into cognitive-communication recovery after traumatic brain injury: A systematic review. International Journal of Speech-Language Pathology, 17, 1-16. https://doi.org/10.1080/17549507.2016.1193896
Elbourn, E., Togher, L., Kenny, B., & Power, E. (2017). Strengthening the quality of longitudinal research into cognitive-communication recovery after traumatic brain injury: A systematic review. International Journal of Speech-Language Pathology, 19(1), 1-16.
Enderby, P., & Palmer. R. (2008). Frenchay Dysarthria Assessment. Texas: ProEd.
Finch, E., Cornwell, P., Copley, A., Doig, E., & Fleming, J. (2017). Remediation of social communication impairments following traumatic brain injury using metacognitive strategy intervention: A pilot study. Brain Injury, 31(13-14), 1830-1839.
Fleming, J. & Strong, J. (1999). A longitudinal study of self-awareness: Functional deficits underestimated by persons with brain injury. The Occupational Therapy Journal of Research, 19, 3-17.
Friedman, I. B., Hancock, A. B.,Schulz, G., & Bamdad, M. J. (2010). Using principles of motor learning to treat apraxia of speech after traumatic brain injury. Journal of Medical Speech-Language Pathology, 18, 13.
Gauthier, S., LeBlanc, J., Seresova, A., Laberge-Poirier, A., Correa, J. A., Alturki, A. Y., Marcoux, J., Maleki, M., Feyz M., & de Guise, E. (2018). Acute prediction of outcome and cognitive-communication impairments following traumatic brain injury: The influence of age, education and site of lesion. Journal of Communication Disorders, 73, 77-90.
Guo, Y. E., & Togher, L. (2008). The impact of dysarthria on everyday communication after traumatic brain injury: A pilot study. Brain Injury, 22,(1), 83-97.
Halliday, M. A. K., & Webster. J. (2009). The essential Halliday. New York; London: Continuum.
Hartley, L. L., & Jensen, P. J. (1992). Three discourse profiles of closed-head-injury speakers: theoretical and clinical implications. Brain Injury, 6(3), 271-281.
Hirstein, W. (2009). Confabulation: Views from neuroscience, psychiatry, psychology and philosophy. Oxford University Press, USA.
Irvine, K.-A., & Clark, J. D. (2018). Chronic pain after traumatic brain injury: Pathophysiology and pain mechanisms. Pain Medicine, 19, 1315-1333. Kaplan, E., H. Goodglass & S. Weintraub. 2001. Boston Naming Test. Texas: ProEd.
Jurado, M. B., & Rosselli, M. (2007). The elusive nature of executive functions: A review of our current understanding. Neuropsychology Review, 17(3), 213-233. doi:10.1007/s11065-007-9040-z
Kaplan, E., Goodglass, H., & Weintraub, S. (2001). Boston Naming Test (Second edition ed.). Proed.
Keegan, L. C., Murdock, M., Suger, C., & Togher, L. (2019). Improving natural social interaction: Group rehabilitation after traumatic brain injury. Neuropsychological Rehabilitation, 1-26.
Kerr, C. (1995). Dysnomia following traumatic brain injury: an information-processing approach to assessment. Brain Injury, 9(8), 777-796.
Kertesz, A. 2012. Western Aphasia Battery-Revised. Texas: Pearson.
Kintz, S., Hibbs, V., Henderson, A., Andrews, M., & Wright, H. H. (2018). Discourse-based treatment in mild traumatic brain injury. Journal of Communication Disorders, 76, 47-59. https://doi.org/https://doi.org/10.1016/j.jcomdis.2018.08.001
Lê, K., Mozeiko, J., & Coelho, C. (2011). Discourse analyses: Characterizing cognitive-communication disorders following TBI. ASHA Leader, 16, 18-21.
Levin, H. S., O'Donnell, V. M., & Grossman, R. G. (1979). The Galveston Orientation and Amnesia Test. A practical scale to assess cognition after head injury. Journal of Nervous And Mental Disease, 167, 675-684.
MacDonald, S. (2017) Introducing the model of cognitive-communication competence: A model to guide evidence-based communication interventions after brain injury. Brain Injury, 31, 1760-1780.
McHenry, M. (2000) Acoustic characteristics of voice after severe traumatic brain injury. The Laryngoscope, 110, 1157-1161.
Merino, R., Pérez, A., Fierro, J., & Terré, R. (2019). Prevalence of medication and off-label medication use in acquired brain injury at a neurorehabilitation hospital. European Journal of Clinical Pharmacology, 75, 985-994.
Metcalf, K., Langdon, R., & Coltheart, M. (2007). Models of confabulation: A critical review and a new framework. Cognitive Neuropsychology, 24(1), 23-47.
Metcalf, K., Langdon, R., & Coltheart, M. (2010). The role of personal biases in the explanation of confabulation. Cognitive Neuropsychiatry, 15(1-3), 64-94.
Meulenbroek, P. A., & Cherney, L. R. (2018). Computerized work-related communication training for persons with traumatic brain injury: User experiences. Archives of Physical Medicine and Rehabilitation, 99(10), e33.
Meulenbroek, P., Ness, B., Lemoncello, R., Byom, L., MacDonald, S., O'Neil-Pirozzi, T. M., & Moore Sohlberg, M. (2019). Social communication following traumatic brain injury part 2: Identifying effective treatment ingredients. International Journal of Speech-Language Pathology, 21(2), 128-142.
Meulenbroek, P., & Turkstra, L. S. (2016). Job stability in skilled work and communication ability after moderate-severe traumatic brain injury. Disability and Rehabilitation, 38, 452-461.
Morton, M. V., & Wehman, P. (1995). Psychosocial and emotional sequelae of individuals with traumatic brain injury: A literature review and recommendations. Brain Injury, 9, 81-92.
Norman, R. S., Jaramillo, C. A., Amuan, M. , Wells, M. A., Eapen B. C., & Pugh, M. J. (2013). Traumatic brain injury in veterans of the wars in Iraq and Afghanistan: Communication disorders stratified by severity of brain injury. Brain Injury, 27, 1623-1630.
Ownsworth, T., & Clare, L. (2006). The association between awareness deficits and rehabilitation outcome following acquired brain injury. Clinical Psychology Review, 26, 783-795.
Parola, A., Bosco, F. M., Gabbatore, I., Galetto, V., Zettin, M., & Marini, A. (2019). The impact of the Cognitive Pragmatic Treatment on the pragmatic and informative skills of individuals with traumatic brain injury (TBI). Journal of Neurolinguistics, 51, 53-62.
Penttilä, N., Korpijaakko-Huuhka, A.-M., & Kent, R. D. (2019). Disfluency clusters in speakers with and without neurogenic stuttering following traumatic brain injury. Journal of Fluency Disorders, 59, 33-51.
Ponsford, J. L., Downing, M. G., Olver, J. H., Ponsford, M., Acher, R., Carty, M., & Spitz, G. (2014). Longitudinal follow-up of patients with traumatic brain injury: outcome at two, five, and ten years post-injury. Journal of Neurotrauma, 31, 64-77.
Ponsford, J. L., Ziino, C., Parcell, D. L., Shekleton, J. A., Roper, M., Redman, J. R., Phipps-Nelson, J., & Rajaratnam, S. M. (2012). Fatigue and sleep disturbance following traumatic brain injury-their nature, causes, and potential treatments. The Journal of Head Trauma Rehabilitation, 27(3), 224-233.
Power, E., Weir, S., Richardson, J., Fromm, D., Forbes, M., Macwhinney, B., & Togher, L. (2020). Patterns of narrative discourse in early recovery following severe Traumatic Brain Injury. Brain Injury, 34(1), 98-109. doi:10.1080/02699052.2019.1682192
Rietdijk, R. (2013). Training communication partners of people with severe traumatic brain injury improves everyday conversations: A multicenter single blind clinical trial. J Rehabil Med, 45, 637-645.
Rietdijk, R., Power, E., Attard, M., Heard, R., & Togher, L. (2020a). A clinical trial investigating telehealth and in-person social communication skills training for people with traumatic brain injury: participant-reported communication outcomes. The Journal of Head Trauma Rehabilitation, 35(4), 241-253.
Rietdijk, R., Power, E., Attard, M., Heard, R., & Togher, L. (2020b). Improved conversation outcomes after social communication skills training for people with traumatic brain injury and their communication partners: a clinical trial investigating in-person and telehealth delivery. Journal of Speech, Language, and Hearing Research, 63(2), 615-632.
Rietdijk, R., Simpson, G., Togher, L., Power, E., & Gillett, L. (2013). An exploratory prospective study of the association between communication skills and employment outcomes after severe traumatic brain injury. Brain Injury, 27(7-8), 812-818. doi:10.3109/02699052.2013.775491
Sarno, M. T. (1980). The nature of verbal impairment after closed head injury. The Journal of Nervous and Mental Disease, 168(11), 685-692.
Seel, R. T., Macciocchi, S., & Kreutzer, J. S. (2010). Clinical considerations for the diagnosis of major depression after moderate to severe TBI. The Journal of Head Trauma Rehabilitation, 25(2), 99-112.
Sherer, M., Katz, D. I., Bodien, Y. G., Arciniegas, D. B., Block, C., Blum, S., Doiron, M., Frey, K., Giacino, J. T., & Graf, M. J. P. (2020). The post-traumatic confusional state: A case definition and diagnostic criteria. Archives of Physical Medicine and Rehabilitation.
Shores, E. A., Lammél, A., Hullick, C., Sheedy, J., Flynn, M., Levick, W., & Batchelor, J. (2008). The diagnostic accuracy of the Revised Westmead PTA Scale as an adjunct to the Glasgow Coma Scale in the early identification of cognitive impairment in patients with mild traumatic brain injury. Journal of Neurology, Neurosurgery & Psychiatry, 79(10), 1100-1106.
Sloan, R., Brown, K., & Pentland, B. (1992). Fluoxetine as a treatment for emotional lability after brain injury. Brain Injury, 6(4), 315-319.
Snow, P., Douglas, J., & Ponsford, J. (1995). Discourse assessment following traumatic brain injury: A pilot study examining some demographic and methodological issues. Aphasiology, 9(4), 365.
Snow, P., Douglas, J., & Ponsford, J. (1997). Procedural discourse following traumatic brain injury. Aphasiology, 11(10), 947-967.
Snow, P., Douglas, J., & Ponsford, J. (1998). Conversational discourse abilities following severe traumatic brain injury: A follow-up study. Brain Injury, 12(11), 911-935.
Snow, P., & Douglas, J. M. (2000). Conceptual and methodological challenges in discourse assessment with TBI speakers: Towards an understanding. Brain Injury, 14(5), 397-415.
Snow, P., Douglas, J. M., & Ponsford, J. L. (1999). Narrative discourse following severe traumatic brain injury: A longitudinal follow-up. Aphasiology, 13(7), 529-551.
Sohlberg, M. M., MacDonald, S., Byom, L., Iwashita, H., Lemoncello, R., Meulenbroek, P., Ness, B., & O'Neil-Pirozzi, T. M. (2019). Social communication following traumatic brain injury part I: State-of-the-art review of assessment tools. International Journal of Speech-Language Pathology, 21(2), 115-127.
Steel, J., Ferguson, A., Spencer, E., & Togher, L. (2017). Language and cognitive communication disorder during post-traumatic amnesia: profiles of recovery after TBI from three cases. Brain Injury, 31(13-14), 1889-1902. doi:10.1080/02699052.2017.1373200
Steel, J., & Togher, L. (2019, 2019/01/02). Social communication assessment after traumatic brain injury: a narrative review of innovations in pragmatic and discourse assessment methods. Brain Injury, 33(1), 48-61. doi:10.1080/02699052.2018.1531304
Tannen, D., Hamilton, H. E., & Schiffrin, D. (2015). The handbook of discourse analysis. John Wiley & Sons.
Togher, L. (2001). Discourse sampling in the 21st century. Journal of Communication Disorders, 34(1-2), 131-150.
Togher, L. (2000). Giving information: The importance of context on communicative opportunity for people with traumatic brain injury. Aphasiology, 14, 365-90.
Togher, L., Hand, L., & Code, C. (1997). Analysing discourse in the traumatic brain injury population: Telephone interactions with different communication partners. Brain Injury, 11, 169-90.
Togher, L., McDonald, S., Code, C., & Grant, S. (2004). Training communication partners of people with traumatic brain injury: A randomised controlled trial. Aphasiology, 18(4), 313-335.
Togher, L., McDonald, S., Tate, R., Power, E., & Rietdijk, R. (2013). Training communication partners of people with severe traumatic brain injury improves everyday conversations: A multicenter single blind clinical trial. Journal of Rehabilitation Medicine, 45, 637.
Togher, L., Wiseman-Hakes, C., Douglas, J. M., Stergiou-Kita, M., Ponsford, J. L., Teasell, R., Bayley, M. , & Turkstra, L. S. (2014). INCOG recommendations for management of cognition following traumatic brain injury, part IV: Cognitive communication. The Journal of Head Trauma Rehabilitation, 29, 353-368.
Tse, W. S., & Bond, A. J. (2004). The impact of depression on social skills: A review. Journal of Nervous and Mental Disease, 192(4), 260-268.
Tu, L. V., Togher, L., & Power, E. (2011). The impact of communication partner and discourse task on a person with traumatic brain injury: The use of multiple perspectives. Brain Injury, 25(6), 560-580.
Turkstra, L., Ylvisaker, M., Coelho, C., Kennedy, M., Sohlberg, M. M., Avery, J., & Yorkston, K. (2005). Practice guidelines for standardized assessment for persons with traumatic brain injury. Journal of Medical Speech-Language Pathology, 13, ix-xxxviii.
Van Borsel, J., Drummond, D., & de Britto Pereira, M. M. (2010). Delayed auditory feedback and acquired neurogenic stuttering. Journal of Neurolinguistics, 23, 479-487.
Van Leer, E., & Turkstra, L. (1999). The effect of elicitation task on discourse coherence and cohesion in adolescents with brain injury. Journal of Communication Disorders, 32(5), 327-349.
Walshe, M. & Miller, N. (2011) Living with acquired dysarthria: the speaker's perspective. Disability and Rehabilitation, 33, 195-203.
Wang, Y.-T., Kent, R. D., Duffy, J. R., & Thomas, J. E. (2005). Dysarthria associated with traumatic brain injury: speaking rate and emphatic stress. Journal of Communication Disorders, 38, 231-260.
Williams, W. H., & Evans, J. J. (2003). Brain injury and emotion: An overview to a special issue on biopsychosocial approaches in neurorehabilitation. Neuropsychological Rehabilitation, 13, 1-11.
Wiseman-Hakes, C., Colantonio, A., & Gargaro, J. (2009). Sleep and wake disorders following traumatic brain injury: A systematic review of the literature. Critical Reviews™ in Physical and Rehabilitation Medicine, 21(3-4).